
Allogene looks to consolidate its position

After a delay, the Alpha-3 study faces an April futility analysis.
After a delay, the Alpha-3 study faces an April futility analysis.
As one of the last players still making a big bet on allogeneic Car-T therapy Allogene has a lot riding on its approach. And, after the company cleared out much of its pipeline, it’s set to deliver a make-or-break dataset next month: first data from the Alpha-3 study of its anti-CD19 contender cemacabtagene ansegedleucel.
This trial tests cema-cel in an unusual setting, namely consolidation in diffuse large B-cell lymphoma patients who are still in response to first-line R-Chop therapy. Unfortunately for Allogene, since the company pivoted to this study two years ago its stock has fallen 25%, though this likely reflects waning investor enthusiasm for allogeneic therapies in general.
It might also show the difficulties faced by any Car-T company in DLBCL, a space that’s been transformed in recent years. Late-line settings have seen the approvals of CD20-targeting T-cell engagers, while the established autologous Car-T therapies Yescarta and Breyanzi now have second-line approvals.
These moves have effectively squeezed out Car-T approaches targeting relapsed/refractory DLBCL, and in the autologous space have seen Caribou shift to an HLA-matching approach, and Precision BioSciences and Adicet abandon oncology entirely. Allogene itself closed trials in third-line DLBCL, but rather than giving up it pivoted to the consolidation approach of Alpha-3.
Genius?
The markets will soon find out whether this was a stroke of genius or whether it, too, is set to fall on stony ground.
Alpha-3 is a phase 2 trial with a pivotal design. It comprises around 220 DLBCL patients who are still in complete or partial response to front-line R-Chop, but who have minimum residual disease (MRD), as determined by Foresight’s Clarity ctDNA test. While the active cohort will get cema-cel, control involves the current standard for such patients of “watch and wait”.
Allogene’s key contention is that simply watching and waiting isn’t good enough, as up to 30% of such patients will require second-line treatment, since the fact they’re MRD-positive suggests that they still have some disease present, even if technically they’ve not progressed.
The aim is for cema-cel to reduce risk of disease recurrence, and in an ideal world to eliminate the need for second-line autologous Car-T therapy. Alpha-3’s primary endpoint is event-free survival, with “events” based on measurements on day 45, month 3 and every three months for the first year.
April’s readout concerns a first futility analysis, based on a comparison of MRD clearance rates between the two cohorts. One mystery is why it’s taken so long to reach this; Alpha-3 started in mid-2024, and all that’s needed to trigger the analysis is the enrolment of 12 patients into each cohort; the analysis had once been expected in mid-2025.
Enrolment might not have been helped by concerns over toxicity: last August Allogene revealed that a patient in Alpha-3 had died. However, it put the death down not to cema-cel but to an enhanced lymphodepletion regimen using its anti-CD52 antibody ALLO-647. Alpha-3 originally tested cema-cel with standard or ALLO-647 lymphodepletion, but after the death all ALLO-647 cohorts were axed.
Benchmark
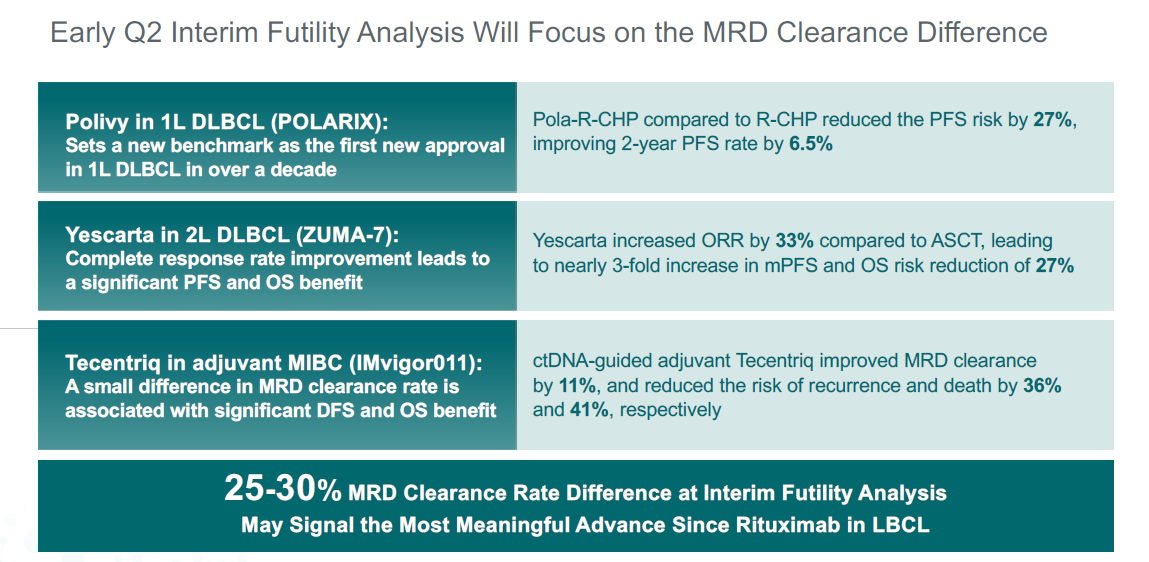
While a statistically significant difference in EFS remains Alpha-3’s ultimate goal the immediate focus falls on MRD clearance; here Allogene has set a benchmark, saying a 25 to 30 percentage point absolute delta between cema-cel and control would represent the “most meaningful advance” in DLBCL since Rituxan.
Allogene expects around 20% of control patients to experience “spontaneous” MRD clearance, amounting to two or three of the 12 subjects, and that’s the baseline against which cema-cel will have to show its 25 to 30-point benefit. Logically it thus figures that Allogene expects six of 12 cema-cel patients to become MRD-negative.
Of course, the interim analysis will formally determine only whether Alpha-3 is futile or if it should continue, but Allogene disclosing such detailed expectations implies that actual MRD numbers will be revealed.
Yet to be determined is whether MRD clearance will amount to an EFS benefit – Allogene has said it’s unclear whether there’s a “linear” relationship between the two – and whether routine MRD status diagnosis will in future be accepted into standard practice. But a hit in April would at least dispel some of the doubts.
2101











